Table of Contents
- Conversion Architecture for Healthcare Pages
- 30-Day Execution Plan
- Common Mistakes and Practical Fixes
- FAQ
Healthcare websites rarely fail because clinics lack medical quality. They fail because patients cannot quickly decide whether this provider is right for them and what to do next. In high-stress situations, even small uncertainty causes drop-off.
A visitor may arrive with strong intent and still leave if service scope is unclear, booking flow is confusing, or trust signals feel generic. This gap affects both patient experience and operational efficiency.
High-performing healthcare web experiences reduce anxiety through clear sequencing. They establish relevance first, credibility second, process clarity third, then provide a low-friction next action.
This guide shows how to implement that system in 2026 with Unicorn Platform. It focuses on decisions that improve qualified bookings, reduce front-desk friction, and create more reliable patient journeys.
sbb-itb-bf47c9b
Quick Strategic Takeaways
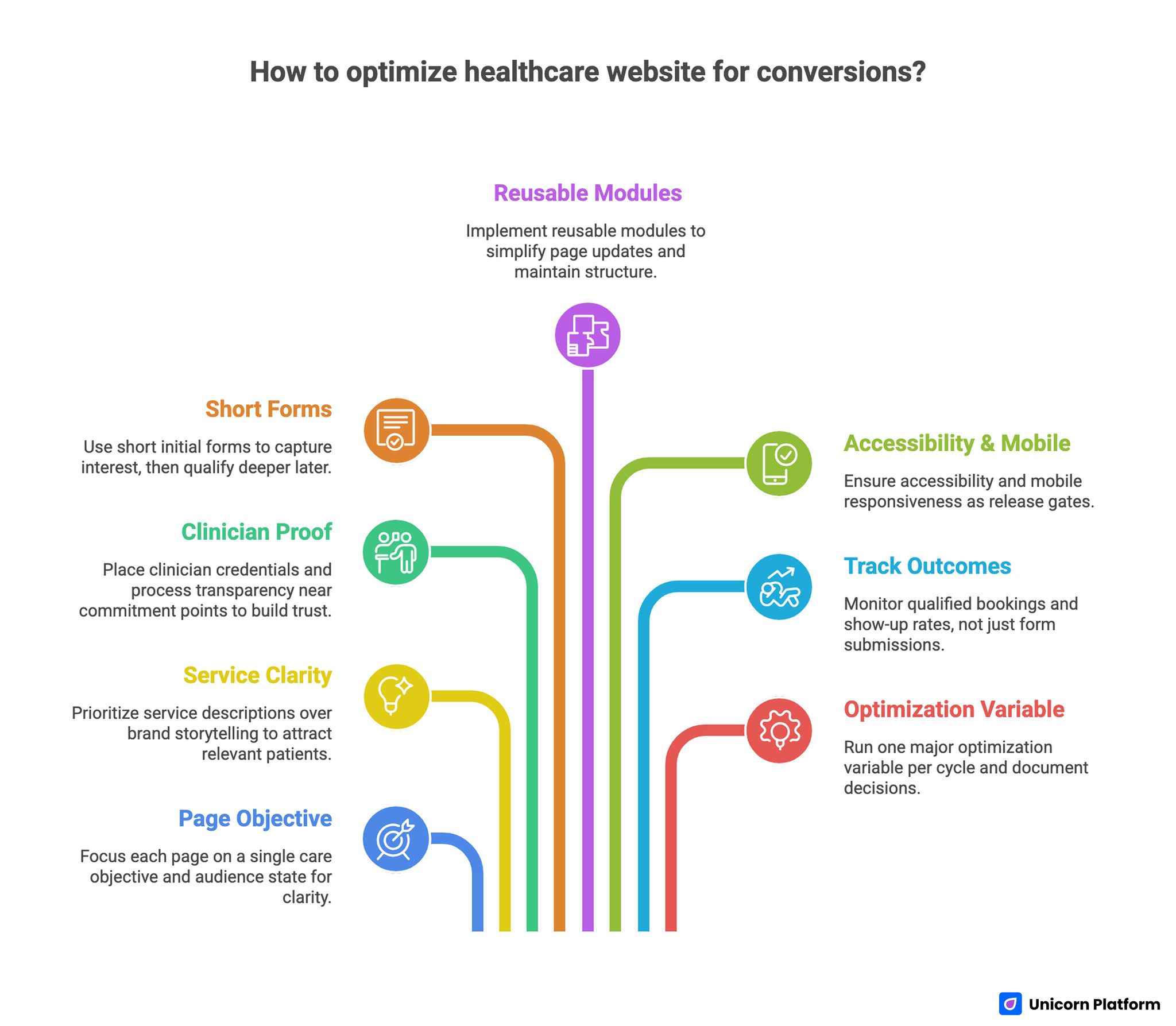
Quick Strategic Takeaways for Optimizing Healthcare Website
- Build each page around one primary care objective and audience state.
- Lead with service clarity and fit cues before brand storytelling.
- Place clinician proof and process transparency near commitment points.
- Keep first-step forms short, then qualify deeper after intent is confirmed.
- Use reusable modules so teams can update pages without breaking structure.
- Make accessibility and mobile interaction quality release gates.
- Track qualified booking and show-up outcomes, not form count alone.
- Run one major optimization variable per cycle and document decisions.
Why Many Medical Websites Underperform
Most underperforming healthcare pages fail in sequence rather than design polish. They open with broad brand claims while patients still need practical orientation.
A patient deciding whether to book wants specific answers immediately: what conditions are supported, who they will see, how soon they can be seen, and what information is needed before the visit. Research shows that a significant portion of patients first seek medical information online before deciding to visit a clinic. According to Pew Research Center, patients evaluate providers based on the clarity of information, accessibility, and straightforward booking steps. When websites fail to provide this quickly, high-intent visitors are more likely to leave or delay their decision. Patients under stress rarely tolerate ambiguity in these areas.
When those answers are delayed, uncertainty rises. High-intent visitors pause, compare alternatives, or leave without contacting the clinic.
The strongest pages reduce that uncertainty in clear stages. Each section should remove one concern and guide users to the next action without forcing extra navigation.
Start With Patient Intent Mapping
Before choosing components, define the page objective in one sentence. Examples include same-week family-practice intake, procedure-specific dental consultations, or specialist referral intake.
Then define patient state. First-time visitors usually need reassurance and process detail. Returning patients often need speed, scheduling access, and clear next steps.
A useful mapping model includes fit criteria, expected timeline, and required preparation. This helps patients self-select and reduces low-fit bookings.
For teams standardizing medical conversion flows, this medical landing page best-practices guide can be used as a structural reference before variant testing.
Intent mapping also helps internal alignment across care, front desk, and marketing teams. Everyone works from one decision model instead of disconnected edits.
Conversion Architecture for Healthcare Pages
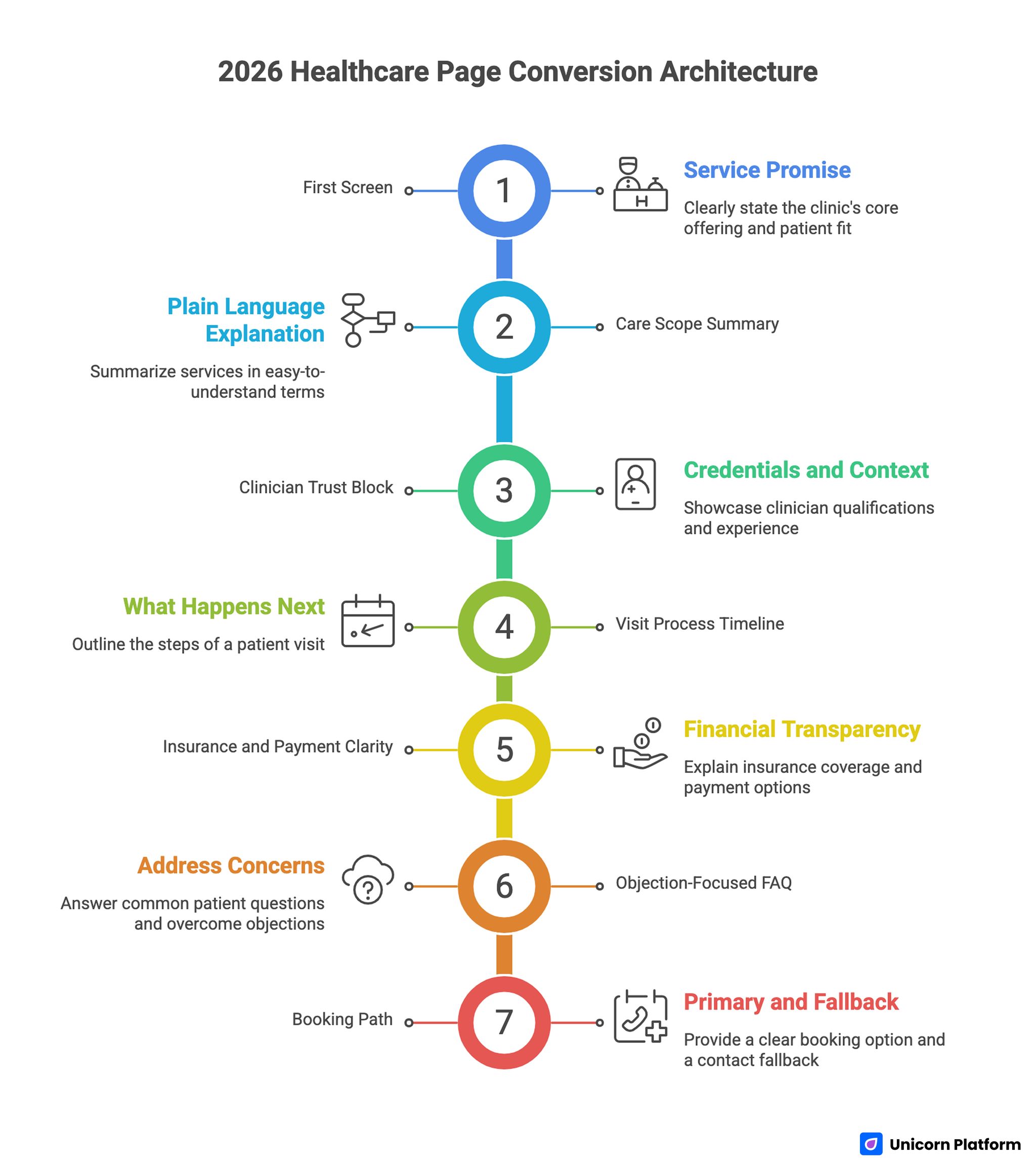
Healthcare Page Conversion Architecture
A durable 2026 healthcare page architecture includes seven modules. This sequence works across family care, dental services, and many specialty paths.
- first-screen service promise with patient-fit qualifier
- care-scope summary in clear, plain language
- clinician trust block with relevant credentials and context
- visit process timeline explaining what happens next
- insurance and payment clarity where relevant
- objection-focused FAQ based on real intake questions
- primary booking path plus secondary contact fallback
This order mirrors patient evaluation behavior. People need relevance and trust before they share personal information.
With Unicorn Platform, teams can reuse this framework across service lines and campaigns while adjusting messaging for local and procedure-specific needs. This keeps campaign execution fast while preserving familiar interaction patterns.
First-Screen Design for Immediate Confidence
The first screen should answer four questions quickly: what care is offered, who it is for, when support is available, and how to begin. If any of these are unclear, many users delay booking.
A practical formula combines service intent, patient qualifier, and one clear action. Vague headlines are weaker than precise language in medical contexts.
CTA labels should match user state. New patients often respond to consultation-oriented actions, while returning patients respond to direct scheduling actions.
Consistency matters across the page. If CTA language shifts unpredictably, users hesitate because commitment expectations feel unclear.
Trust Design: Specific Proof Beats Generic Reassurance
Healthcare trust is earned through specificity. Patients look for clear provider context, relevant experience, and predictable process communication.
A strong trust stack includes clinician credibility, care-process reliability, and patient-outcome context when appropriate. Each signal should be tied to practical concerns patients actually have.
Trust modules are most effective near action decisions, not buried at the bottom. Reassurance should appear where uncertainty spikes.
If your clinic also offers adjacent wellness services, the trust and service segmentation patterns in this med spa strategy guide can help structure specialized landing variants.
Trust content must stay current. Outdated details damage confidence quickly in healthcare settings.
Process Transparency: Tell Patients What Happens Next
Many booking losses come from process ambiguity rather than low intent. Patients want to know response timing, visit format, preparation needs, and follow-up expectations.
Add a short process timeline near booking sections. Keep language simple and concrete.
A high-utility timeline typically includes response window, intake requirements, visit duration expectations, and follow-up process. Clear expectations lower anxiety and improve booking quality.
Process clarity also helps operations. Fewer misunderstandings means fewer corrective calls and better schedule utilization.
Family Practice Page Model
Family practice journeys are relationship-based and often long-term. New patients evaluate continuity, accessibility, and communication style before they commit.
A family-practice page should emphasize care scope, first-visit expectations, and continuity pathways. It should help users understand both immediate and ongoing support.
When teams use the practical method to create family-practice website pages quickly, quality depends on preserving structure while updating local service details and intake realities.
For family care campaigns, splitting first-time and returning-patient paths usually improves both booking speed and fit quality. Each group arrives with different questions and urgency levels.
Dental Conversion Page Model
Dental acquisition often moves fast and is highly procedure-specific. Users compare confidence, cost context, and next-step clarity in a short window.
A dental page should pair treatment-specific framing with immediate process cues. Procedure intent should be clear before long descriptive sections.
When teams use this workflow to build dental clinic landing pages quickly, results improve when each campaign targets one procedure type and one consultation flow.
Procedure-specific variants typically outperform one broad dental page because intent matching is tighter and qualification friction is lower. Clear procedure intent also helps front-desk triage before consultation.
Form Strategy: Balance Speed With Triage Quality
Healthcare forms often fail by asking too much or too little. Oversized first-step forms hurt completion. Under-qualified forms overload staff with weak-fit requests.
A staged approach works best in most cases. Collect essential intent data first, then gather deeper details after initial confirmation.
Field labels should be explicit, and error handling should explain how to recover immediately. Generic error messages are a common abandonment source.
Review form performance with front-desk teams regularly. They have the clearest view of which fields help triage and which create avoidable friction.
Accessibility and Inclusion Standards
Accessibility in healthcare is a core quality requirement, not a secondary enhancement. The World Health Organization emphasizes that digital health services must be accessible and understandable for all patients, including those with disabilities or varying levels of digital literacy. According to World Health Organization, implementing these standards not only increases patient engagement but also improves adherence to care recommendations, which is critical for healthcare quality. Diverse patient populations need reliable readability and interaction clarity.
Baseline standards should include readable typography, high contrast, keyboard support, explicit labels, and actionable error messaging. These standards improve completion for all users, not only edge cases.
In Unicorn Platform, reusable components help teams maintain these standards across frequent updates. Standardization reduces regression risk when multiple contributors publish quickly.
Accessibility checks should be part of every release cycle, not occasional audits. Frequent checks prevent regressions from accumulating between launches.
Mobile and Performance Readiness
A significant portion of healthcare discovery happens on mobile devices. If mobile interaction is weak, high-intent patients may abandon before they reach trust or booking sections.
Release criteria should include first-screen readability, clear CTA visibility, touch-friendly form controls, and reliable contact fallback. These checks should be performed on real devices.
Performance should be judged by action readiness. Users should be able to begin booking without waiting for non-critical assets.
Use mobile regressions as launch blockers in healthcare campaigns. In urgent-care scenarios, interaction delays directly reduce conversion quality.
Measurement Framework for Healthcare Funnels
Submission volume alone is not enough. Strong healthcare optimization tracks outcomes across the full journey.
A practical model includes engagement behavior, booking completion, show-up rate, and post-visit progression signals. This reveals whether campaigns attract the right patients.
Each test should define one primary quality metric and one supporting diagnostic metric. Clear scope makes decisions defensible and repeatable.
Weekly reporting should capture hypothesis, change deployed, observed outcome, and next action. Documentation turns tactical edits into cumulative system improvements.
Operational Governance for Multi-Clinic Teams
Healthcare pages degrade quickly when ownership is unclear. One contributor updates service copy, another adjusts forms, and a third changes policy text without a shared release standard. Over time, this creates inconsistency that patients experience as risk.
A practical governance model assigns four explicit owners. One owner manages service messaging clarity. One owner validates clinical and policy accuracy. One owner maintains conversion performance and analytics integrity. One owner runs release QA for accessibility, mobile behavior, and contact routing.
Teams should maintain one shared change log for every major update. Each entry should capture what changed, why it changed, which metric was expected to move, and what happened after release. This history reduces repeated experiments and accelerates onboarding for new team members.
Governance also improves compliance collaboration. Legal and operations teams can review module-level changes instead of re-reviewing whole pages for small edits. In practice, this shortens publishing cycles while lowering risk.
For organizations managing several specialties, a modular approval matrix is useful. Core trust and policy blocks can require centralized signoff, while localized offer messaging can be approved by regional owners. This balances speed and control.
In Unicorn Platform, this governance model is straightforward because reusable sections can be versioned and deployed consistently. Teams can scale campaign output without sacrificing consistency in patient-facing communication.
30-Day Execution Plan
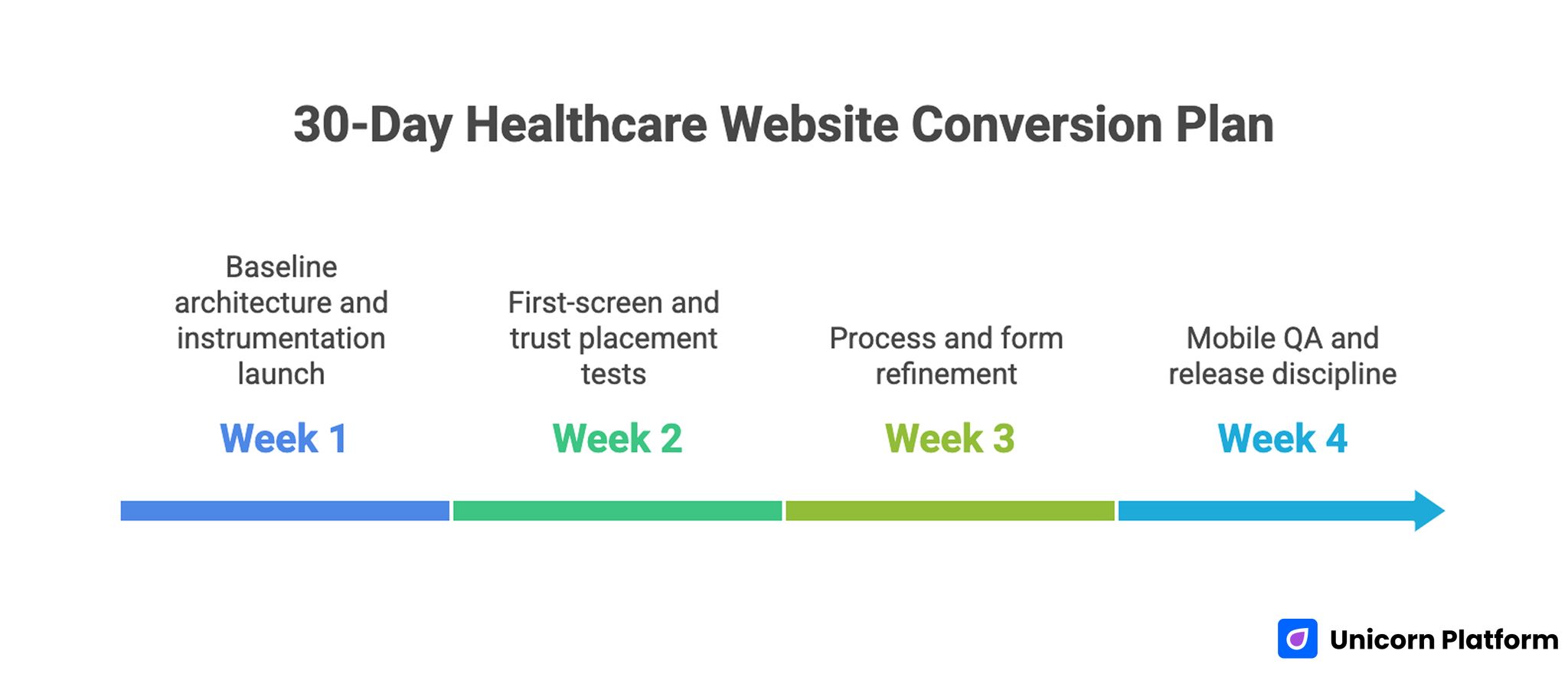
30-Day Healthcare Website Conversion Plan
Week 1: baseline architecture and instrumentation
Launch one service-focused page using the seven-module framework and confirm tracking across key stage transitions. Keep the initial scope narrow to preserve attribution quality.
Capture baseline metrics for completed bookings, qualified intake quality, and intake-call objections. These baselines should be visible in one shared reporting view.
Week 2: first-screen and trust placement tests
Run one first-screen clarity test and one trust-placement test while keeping other variables stable. Limiting concurrent changes reduces interpretation noise.
Evaluate results using booking quality and show-up indicators, not raw form counts. Top-funnel spikes without quality gains should not be scaled.
Week 3: process and form refinement
Improve process timeline clarity and reduce first-step form friction based on front-desk feedback and behavior data. Prioritize changes that remove repeated intake confusion.
Refresh FAQs using the most frequent pre-visit questions from support channels. FAQ language should mirror how patients phrase those concerns.
Week 4: mobile QA and release discipline
Run real-device checks, validate fallback contact routes, and fix interaction regressions before scaling traffic. Document every release blocker and resolution in the same cycle.
Conclude with a keep-change-next memo that defines priorities for the next cycle. The memo should also identify one deferred experiment and the reason for deferral.
90-Day Scaling Model
Scale only after baseline quality stabilizes. Expanding campaign volume on unstable funnels increases operational noise.
Days 1-30 should stabilize architecture and measurement. Days 31-60 should expand service-specific variants with controlled hypotheses. Days 61-90 should convert winning modules into reusable templates and retire weak variants.
This model helps teams move quickly while preserving patient trust, operational clarity, and content consistency. It also reduces campaign drift across service lines.
Common Mistakes and Practical Fixes
Mistake 1: one page trying to serve every service line
Fix by assigning one primary objective per page and routing secondary needs through clearly labeled alternatives. This keeps decision flow simple and measurable.
Mistake 2: generic hero copy with no care-scope clarity
Fix by adding service qualifiers and patient-fit cues in the first screen. Early self-qualification lowers avoidable intake friction.
Mistake 3: trust blocks too far from booking actions
Fix by placing clinician credibility and process reassurance near commitment sections. Reassurance has the most impact at commitment moments.
Mistake 4: unclear post-submit process
Fix by adding a concise timeline that explains response, preparation, and next steps. Process transparency improves booking confidence.
Mistake 5: oversized first-step forms
Fix by collecting essential triage data first and staging deeper intake later. Staged intake usually protects both completion and quality.
Mistake 6: accessibility checks postponed until late
Fix by making accessibility and mobile interaction checks mandatory before launch. These checks should be verified by designated release owners.
Mistake 7: high-volume testing without attribution control
Fix by running one major variable per cycle with explicit hypotheses and measurable outcomes. Controlled scope keeps attribution clean.
Mistake 8: no standardized learning workflow
Fix by maintaining weekly decision logs and updating reusable page modules based on evidence. Documented iteration is what creates compounding gains.
Pre-Publish QA Checklist
Before publishing, run a short QA routine covering clinical clarity, trust, process transparency, and interaction reliability. Keep this checklist embedded in the team workflow so quality checks remain consistent.
Checklist items: Apply this checklist as a release gate for every major update so teams avoid quality drift during fast cycles. Assign one owner to confirm completion before launch.
- service scope and patient-fit cues are clear in the first screen
- primary booking action aligns with campaign intent
- trust and process cues appear near commitment points
- first-step form fields are minimal and triage-relevant
- fallback contact path is visible and tested
- accessibility and mobile checks pass on real devices
- performance supports fast first action
- tracking confirms stage-level funnel measurement
Teams that enforce this checklist usually reduce rework and improve booking quality consistency. Consistent gates also reduce post-launch emergency edits.
FAQ: Healthcare Web Design
How many services should one healthcare campaign page cover?
One primary service objective is usually best for clarity and conversion quality. Secondary services can be linked without competing for primary action.
What matters more than form submissions?
Qualified booking rate and show-up progression matter more because they reflect real operational and revenue impact. Raw submission totals can hide serious fit issues.
Where should trust content appear?
Trust content should appear near booking decisions where hesitation is highest, not only in lower-page credibility sections. Placement is as important as proof content.
Should healthcare forms collect full detail immediately?
Usually no. Staged intake captures core intent first and reduces abandonment while preserving triage quality.
How often should trust and provider details be updated?
Monthly review is a practical baseline, with immediate updates when schedules, services, or staffing details change. Outdated details weaken confidence quickly.
Do service-specific variants improve performance?
Yes, when variants are based on real patient intent differences while keeping structural consistency. Variants should follow behavior data rather than assumptions.
What is a sustainable testing cadence for lean clinic teams?
One major variable per week is usually sustainable and gives cleaner attribution than simultaneous high-volume testing. This cadence also simplifies stakeholder review.
How can clinics reduce low-fit bookings quickly?
Move fit criteria and process expectations higher in the page so patients can self-select before submitting. Early clarity protects both patient time and clinic capacity.
Should educational pages and booking pages stay separate?
They should be connected. Educational pages should route patients to intent-matched booking paths with clear next steps.
What keeps healthcare conversion performance improving over time?
Consistent architecture, stage-based measurement, and documented weekly decisions create durable improvement. Without this discipline, short-term gains usually decay.
Final Takeaway
Healthcare conversion performance improves when pages reduce uncertainty at the right moment. Clear care scope, contextual trust, process transparency, and low-friction booking flow are what turn interest into qualified patient conversations.
Unicorn Platform helps teams maintain this system with no-code speed and reusable structure. When clinical clarity and optimization discipline stay aligned, booking quality improves predictably across services and campaigns.
