Table of Contents
- Decision Model for Behavioral Health Pages
- 30-Day Optimization Cycle
- Scenario Playbooks
- Common Mistakes and Corrections
- FAQ
Behavioral health inquiries are high sensitivity decisions. People who arrive on these pages are often uncertain, overwhelmed, and evaluating whether they can trust the next step.
This means conversion strategy cannot rely on generic growth tactics. Clarity, safety boundaries, and communication reliability matter as much as visual polish.
Teams usually lose performance when they optimize for submission count alone. Strong outcomes come from attracting the right inquiries and preparing people for a realistic intake experience.
This guide lays out a practical system for therapy practices, counseling centers, and behavioral health programs that need faster growth without lowering care trust. It is designed for teams that need repeatable quality, not one-off campaign bursts.
sbb-itb-bf47c9b
Key Takeaways
Key Takeaways for Optimization Behavioral Health Conversion Pages
- Conversion quality improves when fit and scope are explicit in the first screen.
- Trust is built through process clarity, not only testimonials.
- Intake forms should collect routing-critical information first, then expand later.
- Mobile readability and accessibility are core requirements in this category.
- Monthly optimization should track inquiry quality and follow-up reliability, not only top-line volume.
Why These Pages Underperform
Most underperforming pages fail at scope clarity. Visitors cannot quickly tell whether the service fits their concern, urgency, or context.
A second failure point is trust placement. Credentials, confidentiality, and response expectations are often buried below promotional copy.
A third failure point is action friction. Early forms request too much detail before trust is established, which increases abandonment and low-confidence submissions.
A fourth failure point appears post-submit. If response timing and next steps are unclear, people disengage even after completing the form.
Decision Model for Behavioral Health Pages
A reliable page should follow patient decision order rather than internal organizational structure. People typically decide in four stages: fit, trust, process, and action.
Stage one is fit. Visitors need a quick answer on who the service is intended for and what it does not cover.
Stage two is trust. They need reassurance that clinicians, communication protocols, and care boundaries are credible.
Stage three is process. They need practical clarity about what happens after inquiry submission and how matching or triage works.
Stage four is action. Only after those steps are clear should the page push for form completion or booking.
First-Screen Structure That Reduces Anxiety
The opening section should answer four questions immediately: who this service helps, what support looks like, how to begin, and how soon a response can be expected. Missing one of these answers often creates uncertainty that suppresses form completion.
A strong opening combines one specific care-oriented outcome with one process cue. This is more reassuring than broad claims about transformation.
CTA language should remain calm and precise. High-pressure wording can reduce trust in emotionally sensitive decision moments.
For teams standardizing credibility cues and hierarchy across care pages, this healthcare web design operations reference is useful for practical structure checks. It helps keep trust logic consistent when multiple teams publish in parallel.
Trust Architecture for Sensitive Services
Trust in this category is cumulative. One testimonial block is not enough if confidentiality, qualifications, and care process remain unclear.
Use layered trust sections with role-specific credentials, care-method explanation, and communication standards. Each layer should resolve a different uncertainty.
Credential blocks should be concise and relevant. Visitors usually want practical confidence, not exhaustive biography detail.
Communication standards should include response expectations and contact boundaries. Reliability cues often have direct impact on conversion quality.
Responsible Messaging and Claim Safety
Claim language should be evidence-aware and realistic. Overstated promises may increase clicks but often reduce inquiry quality and long-term trust.
Avoid absolute outcomes and vague urgency triggers. Practical, bounded language supports informed decisions and better fit.
When discussing expected progress, include context that outcomes vary by individual needs and treatment path. This protects credibility and reduces mismatch at intake.
For teams calibrating responsible care messaging, the principles in medical conversion page best practices help align clarity with trust. Applying those patterns reduces the risk of overpromising language during campaign updates.
Safety and Crisis Boundary Communication
Every behavioral health inquiry page should define support boundaries clearly. Visitors need to understand what your service can provide and what urgent situations require immediate emergency pathways.
A concise safety block should be visible without heavy scrolling. The tone should be direct, supportive, and non-alarmist.
Boundary clarity is not only a compliance concern. It is a trust signal that shows the organization operates responsibly.
Keep crisis-related content coordinated with regional requirements and internal protocols. Inconsistent guidance across pages can create risk and confusion.
Intake Flow Design for Better Inquiry Quality
First-contact forms should focus on routing essentials. Ask for only the information needed to place a person on the right follow-up path.
Long initial forms can feel invasive in this category, especially before trust is established. Staged intake often performs better and supports safer triage.
Set explicit post-submit expectations near the action button. People should know when they can expect contact and through which channel.
For teams adapting scheduling-heavy workflows, this reservation flow blueprint can help simplify early action without losing process clarity. It is especially useful when teams need to reduce first-step friction quickly.
Service and Product Path Separation
Some organizations run both care services and digital products on adjacent pages. Mixed intent can lower conversion quality if path boundaries are unclear.
Service-oriented paths should prioritize provider fit, care steps, and intake expectations. Product-oriented paths should prioritize usage context, safety boundaries, and support handoff.
Separate these paths while keeping trust language consistent. Path separation reduces misrouted inquiries and improves user confidence.
For product-led behavioral support experiences, this healthcare product page workflow offers practical structure cues. Those cues help teams separate product intent from care-service intent cleanly.
Mobile Readability and Accessibility
Many people access these resources on mobile during difficult moments. Readability and interaction simplicity are therefore conversion-critical.
Use clear typography, high contrast, short section intros, and tap-friendly controls. Dense paragraphs without structure increase drop-off risk.
Accessibility should be part of growth quality, not a later enhancement. Better accessibility often improves clarity for all users.
Validate the full flow on real devices, including form errors and confirmation messages. Desktop previews do not capture many interaction failures.
Channel-Specific Message Alignment
Search visitors often arrive with active need and specific problem language. Referral or social traffic can arrive with lower clarity and higher hesitation.
Keep one core page backbone and adjust opening emphasis by channel. This improves relevance while preserving interpretability across tests.
Paid campaigns should mirror first-screen promise language. Mismatch between ad claim and page reality is a common source of weak inquiry quality.
Referral pathways should reinforce trust transfer cues early. People arriving through partners often expect immediate clarity about professionalism and process.
Post-Submit Continuity and Follow-Up Discipline
A completed form is only the beginning of trust. Conversion quality depends on whether operational follow-up matches what the page promised.
Define response standards and keep them visible in both page copy and confirmation messaging. Clarity after submission reduces anxiety and no-response assumptions.
Review response-timing performance against published expectations. If reality diverges, update either operations or messaging quickly.
For organizations running therapy and adjacent care tracks, this behavioral-health operations framework is useful for keeping message and workflow aligned. Consistent alignment reduces intake confusion and follow-up delays.
Metrics That Predict Real Performance
Submission volume alone can hide quality problems. A more useful model combines volume with care-readiness and operational indicators.
Track qualified inquiry rate, response-time adherence, intake completion, first-session show rate, and reroute frequency. This mix reveals where trust or clarity is failing.
Evaluate metrics by source as well as in aggregate. Aggregate improvements can hide channel-level deterioration.
Run monthly reviews with one major structural change per cycle. Single-variable changes make decisions more reliable.
Governance and Operations Alignment
Behavioral health pages are only as strong as the operational workflow behind them. If page promises and real intake capacity diverge, trust drops quickly even when conversion volume looks healthy.
A practical governance model assigns four owners: clinical messaging reviewer, content editor, operations reviewer, and QA lead. This small structure prevents update drift when campaigns are launched under time pressure.
The clinical reviewer validates scope boundaries and claim safety. The content editor ensures clarity and readability for non-clinical audiences without diluting care accuracy.
The operations reviewer confirms that response windows, communication channels, and route rules match reality. The QA lead validates mobile flow, form behavior, and tracking integrity before publishing.
Run a short pre-publish check with fixed criteria. Fixed criteria are more reliable than open-ended review meetings, especially when teams are busy.
A useful check includes first-screen fit clarity, trust block placement, privacy language accuracy, and post-submit expectation consistency. If one element fails, publish should pause until the issue is corrected.
Keep a lightweight decision log for every major edit. Record what changed, why it changed, and what metric shift you expected.
This log improves handoffs when contributors rotate. It also prevents repeated experiments that previously failed.
Operational alignment should be reviewed monthly with real inquiry outcomes. Pages that convert but create high reroute volume need structural refinement, not more traffic.
When governance stays consistent, teams can scale faster without compromising care quality. This is essential in sensitive categories where trust is the primary conversion asset.
30-Day Optimization Cycle
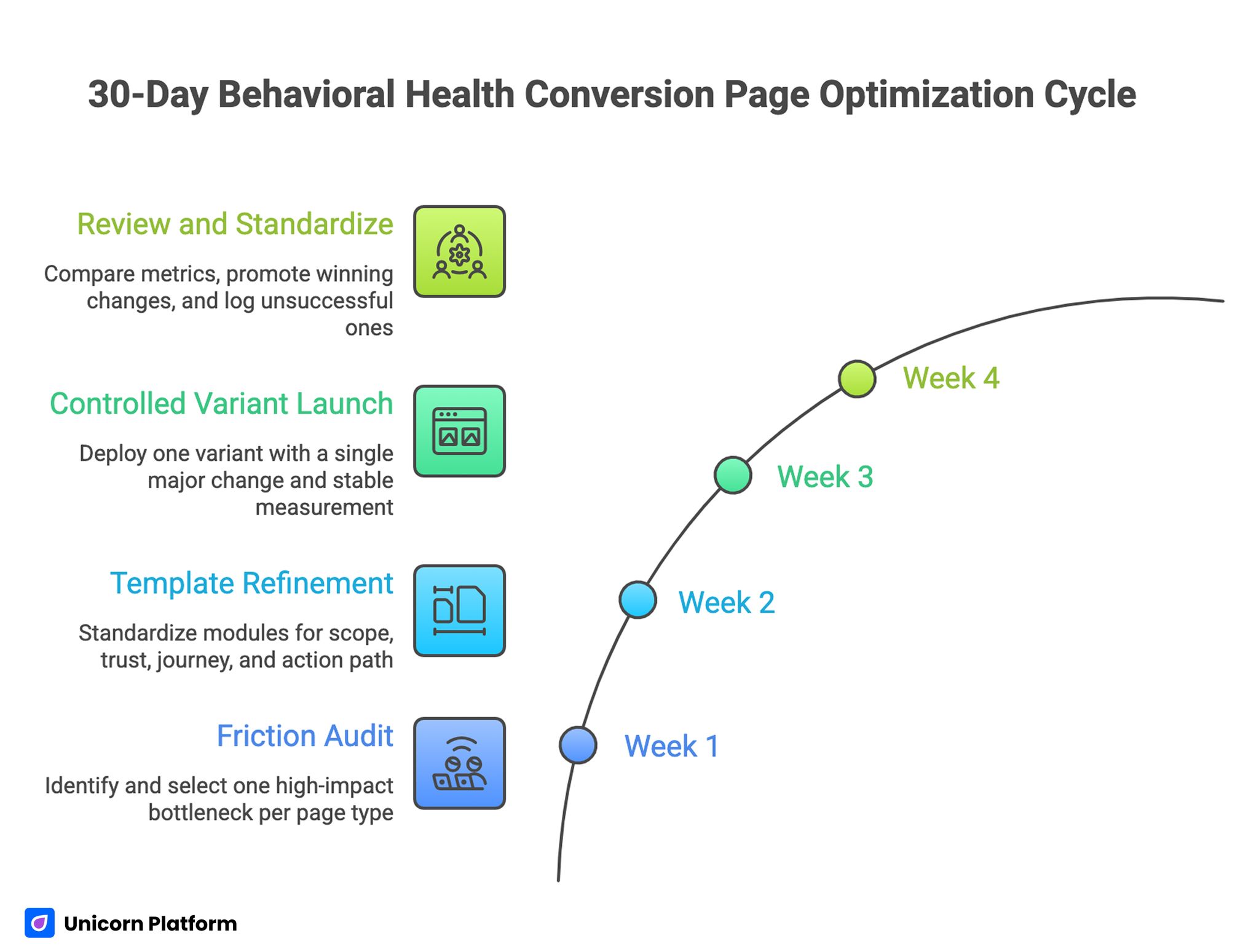
30-Day Behavioral Health Conversion Page Optimization Cycle
Week 1: Friction Audit
Audit top pages for fit clarity, trust placement, intake friction, and mobile readability. Select one high-impact bottleneck per page type.
Week 2: Template Refinement
Standardize modules for scope statement, trust block, journey clarity, and staged action path. Keep module purposes explicit for team consistency.
Week 3: Controlled Variant Launch
Deploy one variant with one major change and a stable measurement window. Avoid simultaneous edits that reduce interpretability.
Week 4: Review and Standardize
Compare quality metrics, promote winning changes to defaults, and log unsuccessful changes with reasons. Repeat monthly with a single objective.
Scenario Playbooks
Scenario A: Strong Traffic, Weak Form Completion
This pattern usually indicates trust gaps or unclear process expectations near the first CTA. Users need reassurance before they share sensitive information.
A practical response is to tighten first-screen scope and move confidentiality plus response details higher on the page. This often improves both confidence and completion quality.
Scenario B: Good Completion, Weak Show Rate
This often signals expectation mismatch before first contact. People convert but are not fully prepared for intake realities.
A practical response is to clarify preparation, response timing, and first-session boundaries before submission. Clear expectations usually improve show rates.
Scenario C: Good Completion, High Reroute Volume
This indicates fit language is too broad and early route cues are weak. Broad language tends to attract mismatched inquiries.
A practical response is to sharpen scope criteria and add explicit pathway guidance in the journey section. Stronger route cues reduce operational handoffs.
Common Mistakes and Corrections
Mistake 1: Broad wellness language without scope
Correction: define who the service is for and what concerns are in or out of scope near the top. Clear scope boundaries improve fit quality quickly.
Mistake 2: Trust elements added late
Correction: place credentials, confidentiality, and process reliability before high-commitment actions. Earlier trust evidence lowers hesitation.
Mistake 3: Intake forms too detailed at first step
Correction: capture only routing-critical fields, then stage additional intake later. This reduces first-step friction while preserving triage quality.
Mistake 4: Outcome claims too aggressive
Correction: use realistic, bounded language and avoid guarantee framing. Responsible phrasing protects long-term confidence.
Mistake 5: Mobile flow validated only on desktop
Correction: test real-device readability, field interaction, and confirmation visibility. Desktop previews alone miss critical behavior issues.
Mistake 6: Optimization focused on volume only
Correction: pair conversion metrics with inquiry quality and operational follow-up indicators. Balanced metrics prevent misleading optimization wins.
FAQ: Behavioral Health Conversion Pages in 2026
1) What should these pages communicate first?
Start with fit and scope. People need immediate clarity on whether the service is relevant before they evaluate deeper details.
2) How much trust information should appear above the first CTA?
Include enough to reduce core risk perception: role credibility, confidentiality cue, and process expectation. These elements support informed decisions before submission.
3) Should confidentiality language be near forms?
Yes. Privacy confidence near action points can materially improve completion quality.
4) What is the best initial form length?
Keep first-step forms short and routing-focused. Additional details can be gathered in later steps.
5) How do we reduce no-shows from page-driven inquiries?
Set clear expectations for response timing, preparation, and first-session flow before submission. Better expectation framing reduces no-shows and confusion.
6) Can service and product paths share one page?
They can share trust framework, but action paths should be separated to avoid user confusion. Intent separation improves routing accuracy.
7) Which metric should teams watch first?
Qualified inquiry rate paired with response-time adherence gives a strong early signal of quality. This pair captures both fit and operational reliability.
8) How often should we optimize these pages?
Use monthly structured cycles with one major change each time for clean learning. Controlled cadence improves interpretability and team focus.
9) What is the fastest high-impact improvement?
Rewrite first-screen fit language and add visible process expectations near the first CTA. This is often the fastest high-impact improvement.
10) How do we maintain consistency across regions or teams?
Use standardized trust modules and a mandatory QA check before launch. Standardization helps teams scale safely across regions and service lines.
Final Takeaway
Behavioral health conversion pages perform best when trust, scope clarity, and operational reliability are designed as one system. Better performance in this category means better-fit inquiries and smoother care pathways, not only higher form counts.
Teams that run structured trust modules, staged intake flow, and disciplined monthly optimization can scale demand while protecting patient confidence and care readiness. This balance is what makes growth sustainable in behavioral health services.