Table of Contents
- Build the Page Around Patient Decision Stages
- 30-Day Healthcare Optimization Cycle
- Scenario Playbooks
- Common Mistakes and Corrective Actions
- FAQ
Healthcare marketing has a narrower margin for error than most industries. People are not just comparing convenience and price. They are evaluating safety, credibility, and confidence in what will happen after they submit a form.
This is why page polish alone is not enough. A page can look professional and still fail if users cannot quickly understand service fit, care process, provider credibility, and expected response timeline.
Strong healthcare conversion outcomes come from structured clarity. Visitors need to move from uncertainty to informed action without being pushed into premature commitment.
This guide presents a complete operating model for clinics, multi-service providers, and health products teams that need better inquiry quality with lower operational friction. The focus is practical execution, not generic marketing advice.
sbb-itb-bf47c9b
Key Takeaways
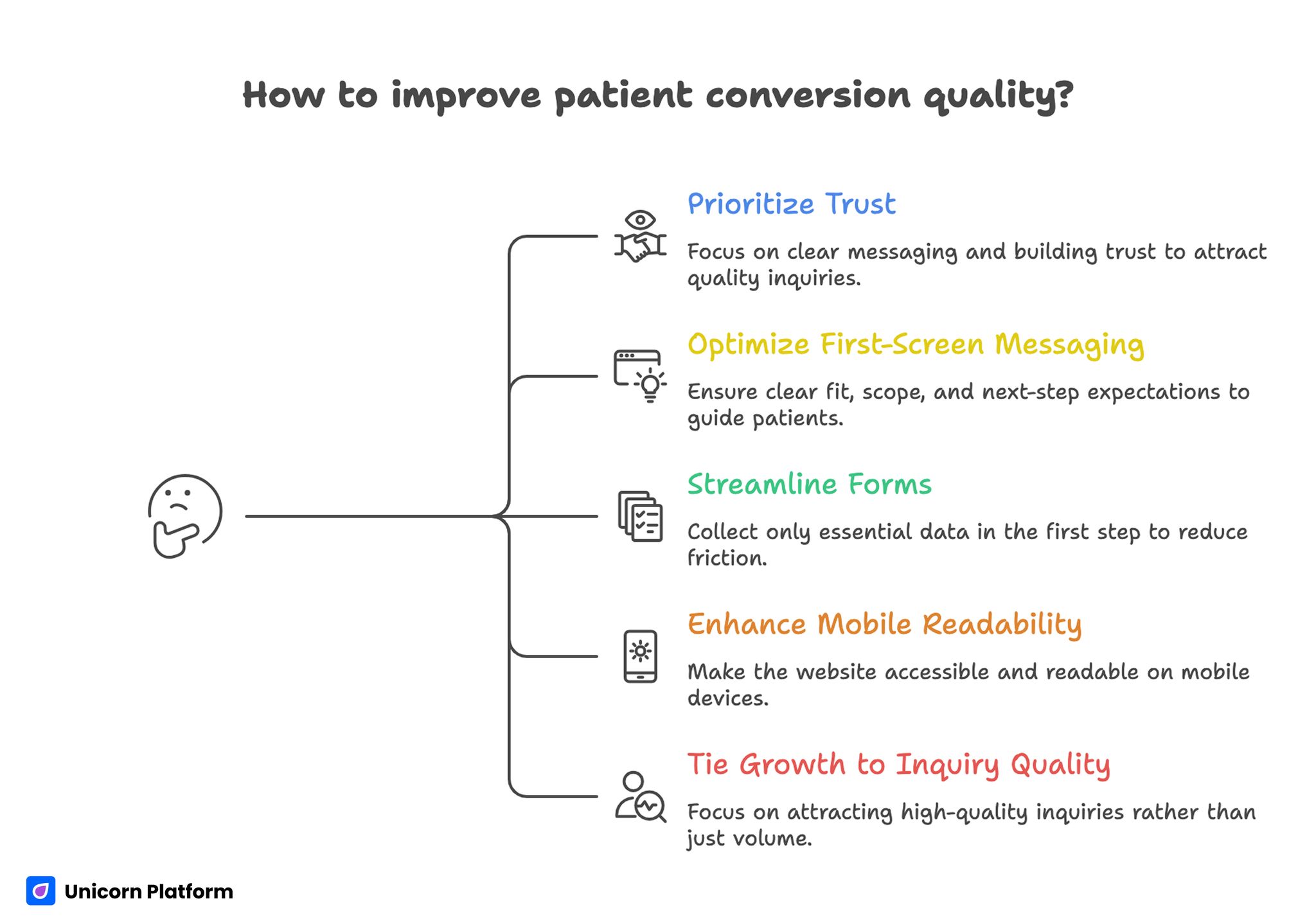
Key Takeaways for Improving Patient Conversion Quality
- Patient conversion quality depends on trust clarity more than visual style.
- First-screen messaging should prioritize fit, scope, and next-step expectations.
- Forms should collect only routing-critical data in the first step.
- Mobile readability and accessibility are core conversion requirements.
- Growth decisions should be tied to inquiry quality, not submission volume alone.
Why Healthcare Pages Underperform
Most weak pages fail because they describe services too broadly. Visitors read general language but still cannot determine whether the offer fits their specific situation.
A second problem is buried trust information. Provider credentials, care process details, and communication standards often appear too late in the page to reduce early hesitation.
A third problem is intake friction. Teams request too much information before trust is established, which lowers completion and increases partial inquiries.
A fourth problem appears after form submission. When response expectations are unclear, users lose confidence quickly even if they already converted.
Build the Page Around Patient Decision Stages
A reliable healthcare page should follow the order patients use to decide. People first check relevance, then safety, then process clarity, and only then commitment.
Stage 1: Fit and Scope
Start with who the service is for and what it addresses. Clear scope statements help users self-qualify and reduce low-fit submissions.
Stage 2: Trust and Credibility
After fit, show why your team is credible. Credentials, care standards, and communication commitments should be visible before action prompts.
Stage 3: Process Expectations
Explain what the first interaction includes, how long responses take, and what information is needed. Process clarity lowers anxiety and increases completion quality.
Stage 4: Action Path
Only after relevance, trust, and process are clear should the page emphasize form completion or booking action. This ordering protects quality while improving conversion confidence.
First-Screen Structure for Healthcare Contexts
The opening section should answer four questions in under ten seconds. Visitors need to know who you help, what kind of support you provide, how to start, and what happens after request submission.
A strong opening block combines a precise service statement with one confidence cue, such as provider context or response standard. This structure is usually more effective than broad claims about excellence.
CTA wording should match patient readiness. High-pressure language can reduce trust in care-oriented environments where users need reassurance and clarity.
For teams refining core structure and visual trust signals, this healthcare web design operations reference is useful when mapping first-screen priorities. It helps teams keep credibility cues consistent across service categories.
Trust Architecture That Supports Conversion
Trust in healthcare is not created by one testimonial section. It is created by consistent evidence across page sections.
Use a layered trust model with provider credibility, process transparency, and communication reliability. Each layer should answer a different patient concern.
Provider credibility should include relevant qualifications and care context. Process transparency should explain how care is delivered and what the first step looks like.
Communication reliability should set expectations for response channels and timing. Reliable communication cues often influence conversion as much as clinical detail.
Responsible Claim Language
Healthcare claims should be specific, cautious, and evidence-aware. Overstated promises can increase initial clicks while weakening long-term trust and conversion quality.
Use realistic phrasing around outcomes and timelines. Where outcomes vary by patient context, state that clearly and early.
Avoid guarantee-style language unless it is legally and clinically supportable. Responsible language improves both compliance safety and user confidence.
When teams combine trust architecture with responsible claim design, inquiry quality improves and intake misunderstandings decline. This combination protects both conversion performance and patient confidence.
Patient Journey Clarity Blocks
Patient journey sections should explain the path from inquiry to first care interaction. Users convert better when they understand sequence, effort, and expected timing.
A practical journey block includes three components: initial request step, follow-up contact step, and first assessment step. This keeps expectations grounded without overwhelming visitors.
If multiple service paths exist, include brief route distinctions. Clear route guidance reduces rerouting workload for care and support teams.
Journey clarity is especially important for new visitors who may not know clinical terminology or intake expectations. Clear sequencing reduces uncertainty before they reach the form.
Intake Form Design for Quality and Completion
The first form should collect only information needed for safe routing and follow-up. Extra fields can be added later in staged intake workflows.
Shorter initial forms usually increase completion without reducing quality when routing logic is well designed. Excessive early fields often produce abandonment and lower confidence.
Use plain field labels and explicit privacy cues. Patients are more likely to complete forms when they understand why each field is requested.
Set clear post-submit expectations near the submit button. Users should know when they will hear back and through which channel.
For services that require appointment-style flow, this reservation pathway blueprint can help structure lower-friction action blocks. Use it to simplify decision steps without losing process clarity.
Service Pages vs Product Pages in Healthcare
Many healthcare organizations now publish both care-service pages and product-focused pages. Conversion quality drops when these intents are blended without clear boundaries.
Service pages should prioritize patient fit, care process, and provider context. Product pages should prioritize usage guidance, suitability boundaries, and next-step clarity.
When both intents are relevant, use separate paths with shared trust framework. Intent separation reduces confusion and improves downstream routing quality.
For teams building product-focused variants, this healthcare product page workflow is practical for aligning clarity and trust. It is especially useful when service and product intents coexist.
Mobile and Accessibility Standards
Healthcare browsing frequently happens on mobile, often during stressful decision windows. Pages must remain clear under limited attention and time.
Use readable typography, strong contrast, short section intros, and tap-friendly controls. Dense blocks and ambiguous buttons reduce comprehension on small screens.
Accessibility should be treated as a conversion requirement, not a secondary enhancement. Better accessibility often improves action completion for all users.
Test full mobile flow including form errors, confirmation state, and contact visibility. Real-device checks catch issues desktop previews miss.
Channel Alignment for Healthcare Campaigns
Different acquisition channels carry different expectation levels. Search traffic often arrives with specific problem intent, while social traffic may require faster trust reinforcement.
Keep one core page structure and adjust opening emphasis by source. This preserves operational consistency while improving message match.
Paid campaigns should align ad language with first-screen promise. Message mismatch is a common cause of high click volume with weak inquiry quality.
Referral traffic should include clearer trust transfer cues. Visitors from partner sources often expect immediate credibility confirmation.
Post-Submit Continuity and Follow-Up Reliability
Conversion quality depends on what happens after submission. Weak follow-up reliability can erase trust even when form completion improves.
Define a follow-up standard and communicate it clearly on-page and in confirmation messaging. Consistent expectations reduce anxiety and lower support burden.
Align page promises with real operational capacity. Overstating response speed can increase early submissions but damage long-term confidence.
For teams running behavioral-health pathways, this mental health page operations guide helps maintain continuity between message and care workflow. Consistent pathway language lowers follow-up confusion.
Metrics That Predict Real Healthcare Value
Submission count alone is not enough. Strong healthcare pages are measured by inquiry quality and care-path fit.
Use a balanced metric model. These five indicators keep volume and quality interpretation aligned:
- qualified inquiry rate,
- response-time adherence,
- appointment show rate,
- reroute frequency,
- first-visit completion quality.
This model reveals whether page messaging attracts the right patients and sets accurate expectations. It also shows where operational fixes are needed.
Review results monthly and optimize one major structural variable at a time. Controlled iteration produces cleaner learning than broad redesign waves.
Add one cross-team alignment check to each monthly review. Clinical operations, support, and marketing should confirm that page promises still match real intake capacity, because conversion quality drops quickly when message timing and staffing realities diverge. This small check often prevents expensive campaign misalignment.
30-Day Healthcare Optimization Cycle
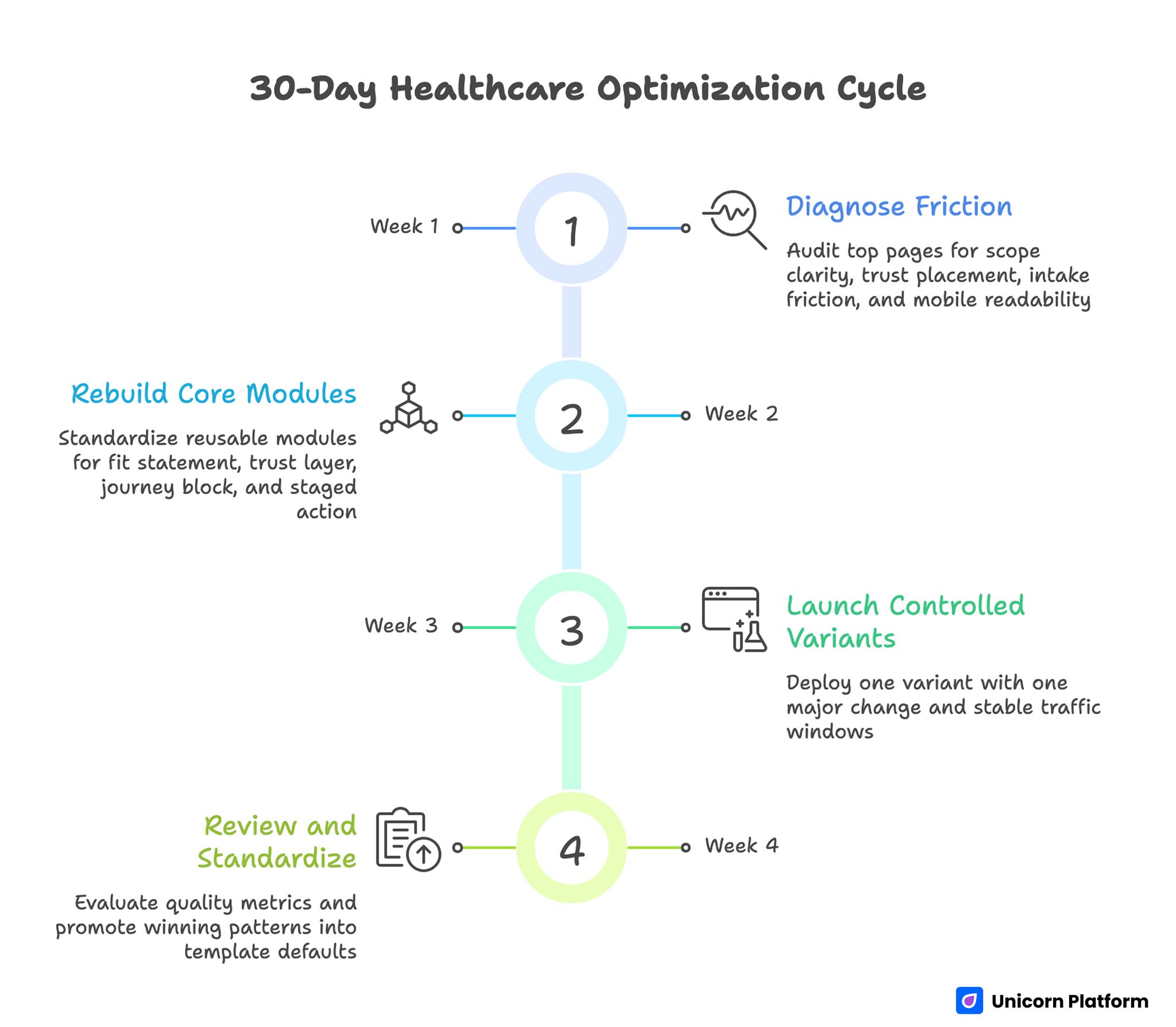
30-Day Healthcare Optimization Cycle
Week 1: Diagnose Friction
Audit top pages for scope clarity, trust placement, intake friction, and mobile readability. Identify one high-impact bottleneck per page type.
Week 2: Rebuild Core Modules
Standardize reusable modules for fit statement, trust layer, journey block, and staged action. Keep module job definitions explicit for cross-team consistency.
Week 3: Launch Controlled Variants
Deploy one variant with one major change and stable traffic windows. Avoid simultaneous structural and messaging changes that reduce interpretability.
Week 4: Review and Standardize
Evaluate quality metrics and promote winning patterns into template defaults. Archive losing variants with short notes to prevent repeat mistakes.
Repeat monthly to keep pages aligned with patient behavior and operational realities. Regular cadence prevents gradual trust decay across campaigns.
Scenario Playbooks
Scenario A: High Traffic, Low Completion
Users reach the page but avoid submitting. This often indicates weak trust placement or unclear care process expectations.
A practical response is to strengthen first-screen scope clarity and move process transparency closer to the first CTA. This usually improves both confidence and completion.
Scenario B: Good Completion, Low Show Rate
Form submissions look strong, but appointment attendance is weak. This usually indicates expectation mismatch in pre-visit messaging.
A practical response is to clarify response timelines, visit preparation, and suitability boundaries before form submission. Better expectation design often improves attendance quality.
Scenario C: Good Completion, High Reroute Volume
The page converts, but many inquiries route to the wrong service line. This pattern signals weak fit criteria in early sections.
A practical response is to tighten service scope language and add clear route cues in the journey block. Stronger routing cues reduce unnecessary operational handoffs.
Common Mistakes and Corrective Actions
Mistake 1: Generic service descriptions
Correction: use precise fit language and practical scope boundaries in the first two sections. Fit clarity lowers low-intent submissions.
Mistake 2: Trust cues placed too late
Correction: move credentials and process reliability information higher in decision flow. Earlier trust signals reduce hesitation.
Mistake 3: Long first-step forms
Correction: stage intake and collect only routing-critical information initially. Additional detail can be captured after contact.
Mistake 4: Overstated outcome claims
Correction: use evidence-informed language with realistic expectation framing. Responsible phrasing protects long-term trust.
Mistake 5: Weak mobile readability
Correction: validate typography, CTA clarity, and form behavior on real devices before launch. Real-device checks catch critical usability gaps.
Mistake 6: Optimizing for volume only
Correction: pair conversion metrics with quality indicators like show rate and reroute frequency. Balanced metrics prevent misleading wins.
FAQ: Healthcare Conversion Pages in 2026
1) What should healthcare pages communicate first?
Start with who the service is for and what support it provides. Immediate fit clarity improves qualified action rates.
2) How much trust content is enough?
Include enough proof to resolve core safety and credibility concerns before the main action. Trust depth should match decision risk.
3) Should provider credentials be near the top?
Yes, when they are relevant to the offered care path. Early credibility cues usually reduce hesitation.
4) What is the best first form length?
Use the shortest form that still supports safe routing and follow-up. Additional intake can happen after first contact.
5) How can teams reduce no-shows from landing traffic?
Set clear pre-visit expectations for timing, process, and preparation before submission. Transparent expectations reduce preventable no-shows.
6) Should care services and products share one page?
Only if intent paths are clearly separated. Mixed goals without boundaries reduce conversion quality.
7) Which metric should teams track first?
Track qualified inquiry rate with response-time adherence. That pair gives fast insight into both fit and execution.
8) How often should these pages be reviewed?
Run monthly structured reviews with one major optimization change per cycle. Single-change cycles improve interpretability.
9) What is the fastest high-impact improvement?
Rewrite first-screen scope and add visible process expectations near the primary CTA. This fix usually improves quality quickly.
10) How do teams keep trust consistent across campaigns?
Use reusable trust modules with standardized language and mandatory QA checks before launch. Standardization helps teams scale safely.
Final Takeaway
Healthcare conversion performance improves when clarity, trust, and operational reliability are designed as one system. Better pages do not just generate more submissions; they generate better-fit inquiries with stronger downstream care outcomes.
Teams that apply structured trust architecture, staged intake flow, and monthly evidence-based optimization will build more stable growth without sacrificing patient confidence. That discipline also improves coordination between marketing and care operations.